




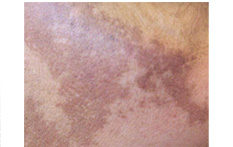
Melasma on face during pregnancy
Melasma is a common acquired progressive non scaling hyper pigmentation disorder that affects sun-exposed areas of the skin. It is characterized by arcuate or polycyclic hyperpigmented light-brown to gray-brown macules and patches involving the face, especially the cheeks, central face forehead, upper lips, nose, bridge of the nose, and chin, more frequently seen around the eyes. The dark brown, symmetric patches of pigment on the face are similar in appearance to age spots but with larger areas of darkened skin. It also can appear on other parts of the body that get lots of sun, such as the dorsal forearms and neck.
Melasma typically presents in one of three patterns of distribution: centrofacial (63%), malar (2%), and mandibular (16%). It is usually, but not always, bilateral.
Three types of melasma exist: epidermal, dermal, and mixed. Determining whether the patient has dermal vs. epidermal melasma will affect therapy, as the dermal form is not likely to respond to bleaching agents. Melasma may appear brown or blue depending on the depth of the pigmentation, either epidermal or dermal, respectively.
Epidermal melasma tends to be light brown, enhancing under Wood lamp examination. The epidermal type characteristically has increased melanin in the basal and suprabasal layers, with some basal-layer vacuolization. This is the most common as well as the most treatable type of melisma.
Dermal melasma is usually grayish in color and nonenhancing. Mixed types are dark brown with variable enhancement. The so-called Tyndall effect accounts for the blue appearance of dermal melasma. This is due to melanin’s absorption of light and the refractive properties of light itself, which lead to its subsequent dispersion and re-emergence with a perceived blue hue. If a Wood’s lamp examination is equivocal, then a biopsy may be necessary to distinguish the two.
This disorder can occur during pregnancy and is sometimes referred to as the "mask of pregnancy." It is usually related to hormone excess, as in pregnancy, oral contraceptive pill use, and endocrine disorders. In women taking oral contraceptives, about 30% develop melasma because their bodies undergo similar kind of hormonal changes that occur during pregnancy. Melasma of the upper lip is a marker for oral contraceptive pill use. It may also be associated with some other medications and severe liver disease, or it could be idiopathic.
Other factors that may contribute to its formation are the combination of sun damage and the use of certain products, such as deodorants, toiletry and other personal care items to which a person has a sensitivity.
The pathogenesis of melasma is unclear. Some investigators have suggested that betalipotropin secreted by the pituitary gland may induce melasma. It is a known melanotropic peptide. However, this has yet to be proven, as levels of the protein are not altered between those affected and controls.
Melasma is clearly affected in some way by estrogen or progesterone, given the temporal relationship of onset to pregnancy and ingestion of birth control pills. Studies of melasma in men have also implicated subtle hormonal imbalances as a possible mechanism for its pathogenesis. Interestingly, women who are postmenopausal and on estrogen therapy do not usually have melasma. However, if the woman is given hormone replacement therapy that contains progesterone, she is likely to get melasma. This implicates progesterone as a key mediating hormone in melasma induction.
Melasma is not exclusively a disorder of ethnic populations, studies of the epidemiology of melasma reveal it to be a common disorder among darker-skinned races. It is more prominent in patients with skin types IV to VI. It is frequent among Middle Eastern, Latinos, African-Americans and Africans (particularly Ethiopians) as well as Asians and Pacific islanders. Clearly, there is a genetic predisposition to the development of melasma, as it can be seen in mothers of the same family as well as in twins. Melasma can also occur in men, but males compose only 10% of cases.
Sunscreens and avoiding sun exposure can prevent melasma from becoming worse. Other treatment may include prescription creams to lighten the patches. One of the most common treatments for melasma is sun protection. This means wearing sunscreen every day and reapplying the sunscreen every 2 hours. Dermatologists also recommend wearing a wide-brimmed hat when you are outside. Sunscreen alone may not give you the protection you need. .. In the case of hormonal-induced melasma, once childbirth has occurred or the use of oral contraceptives has been discontinued, the condition usually will dissipate on its own.
>
>
>
>
>
>
>
>
>
>
>
>
>
>
>
>
>
>
>
>
>
>
>
>
>
>
INTRODUCTION
PIGMENTARY DISORDER TYPES
Disorders of
Hyperpigmentation
Disorders of Hypopigmentation
COMMON PIGMENTARY DISORDERS
Age Spots/Liver Spots/Lentigos
Acanthosis Nigricans
Albinism
Cafe-au-Lait Macules
Ephelides (Freckles)
Erythema Dyschromicum Perstans (Ashy Dermatosis)
Familial Racial Periorbital Hyperpigmentation
Idiopathic Guttate Hypomelanosis
Leopard Syndrome
Linea Nigra
Melanoma
Melasma
Nevus (birthmarks/moles)
Parkinsons Disease
Phytophotodermatits
Pityriasis Alba
Poikiloderma of Civatte
Postinflammatory
Hyperpigmentation & Hypopigmantation
Seborrheic Keratoses
Sturge-Weber Syndrome
Substance Induced
Hypermelanosis
Tinea Nigra/Tinea Versicolor/Pityriasis
Versicolor
Vitiligo
Waardenburg Syndrome

<< Previous: Melanoma
Next: Nevus (Birthmarks /Moles)>>